The CDC: Source of Misinformation
One lasting casualty of the COVID-19 pandemic is lost trust in public health. The CDC recently lifted their recommendation for mask mandates, following nearly all governors already lifting them.
It reminded me of a scene in Beverly Hills Cop. Axel Foley had disarmed one robber, and Sergeant Taggart had disarmed the other. When it was over, in stormed Billy Rosewood, shouting “Don’t move! Turn over!” And he put the cuffs on the bad guy. Foley turned to him and said, “Way to go Rosewood.”
Way to go CDC.
It’s very puzzling why the CDC, most in the media and in the medical community hung on to many COVID-19 restrictions when the data was so apparent they didn’t suppress COVID-19. The lasting impact of this will be distrust in public health and those in the media. For example, I’m no expert on climate change.
However, will anyone look at a report that says “97% of scientists agree…”, or a headline that reads “According to experts…” the same again? After all of this, everyone should fact check any “expert” analysis for themselves with two to three sources before running with it.
The CDC is not a policy maker but the most important policy influencer. The CDC failed on so many pandemic recommendations it’s hard to count. Here are a few, and no doubt books will be written on this topic alone:
- Not supporting outdoor activities at all times and ever endorsing wearing face masks outdoors.
- Remote learning in the fall of 2020 and beyond.
- Face masks required in schools.
- Social distancing in schools, thus reducing capacity in classrooms and requiring remote learning.
- Toddlers wearing face masks in day care.
- Closing indoor dining, gyms and many retailers.
- Eliminating “elective” surgeries. These weren’t face lifts halted. These were actual surgeries, cancer diagnoses, treatments, and so many more.
- Vaccinating healthy young people, rather than emphasizing those over fifty, or overweight or with other select underlying conditions be vaccinated.
- mRNA doses should have been spaced out more than 21 days, particularly for young people.
- Parsing out vaccination recommendations. For example, young healthy men, if they got one, were better off with the J&J than a mRNA; healthy women under fifty would be better off without the J&J; people under thirty or so should stay away from the Moderna vaccine, and many other tailored recommendations. The data as of spring 2021 supported all these stratifications.
- Not recommending recovered infection immunity as equivalent to having received the vaccines.
- The CDC changed their official definition of a vaccine to conform with the COVID-19 vaccines, rather than accept that the COVID-19 vaccines were more therapeutic in nature than what we have come to expect from a vaccine. There is nothing wrong with that. It seems consensus that the vaccines provide some protective benefit, and have more side effects than other vaccines. Those are near-facts as of 2022 (and were by early 2021), and there is nothing wrong with saying so.
As of late 2021, 78% of Americans polled believed at least one commonly communicated COVID-19 policy or reporting was false. The CDC cried wolf and jumped the shark so many times that they lost a chunk of the population when it counted. The CDC did not commission a single randomized clinical trial on face masks nor therapeutics. They had one strategy that never evolved: close public places, wear face masks, and everyone get vaccinated.
There is no doubt they have lost the trust of many if not most Americans. However, this is not an existential loss in trust. Anytime you hear about something being an existential anything, dismiss it. People, trust, democracy…these things are resilient. Regaining trust in the CDC and public health will require:
- Leadership change.
- Acknowledgment that pandemic recommendations became misguided.
- A few years of consistent quality, actual science-based work output.
Below is an excerpt from COVID-19: The Science vs. The Lockdowns:
Jumping The Shark
Then it happened. We reached our peak. But like the COVID-19 waves, there were three peaks. The CDC gets credit for all three of these distinctions. It’s disheartening to pick on the CDC because there are some brilliant doctors and scientists that do incredible work. Still, it’s clear after COVID-19 the leadership needed an overhaul. They jumped off the mountain of public healthcare three times and flew off in a wing suit of zero-COVID-19. If you follow extreme sports, you know how dangerous that can be. Just look up climbing great Dean Potter.
I watched Happy Days as a little kid. Before the expression of jumping the shark became a commonplace term, seeing Fonzie jumping a shark on water skis wearing a leather jacket real-time was just too much. Businesses created products that jumped the shark. Many television shows have done it. You’ve probably had a dinner party when someone made a comment so over the top you had to look down to see if they were wearing water skis.
The CDC did it with two different directors.
Dr. Robert Redfield seems like a nice enough man. He achieved his undergraduate and doctorate degrees at Georgetown. He served as a doctor in the U.S. Army and was distinguished through his work in immunology and virology. No tone in this, Redfield must be very bright. Fast forward to 2018 when he was appointed director of the CDC. He came into this role with the healthcare crisis of generations in front of him. The CDC was the first to proclaim wearing masks was necessary to curb COVID-19 transmission in the spring of 2020.
On September 16, 2020, Dr. Redfield spoke to a Senate committee. While holding up a disposable surgical mask (below), he said this:
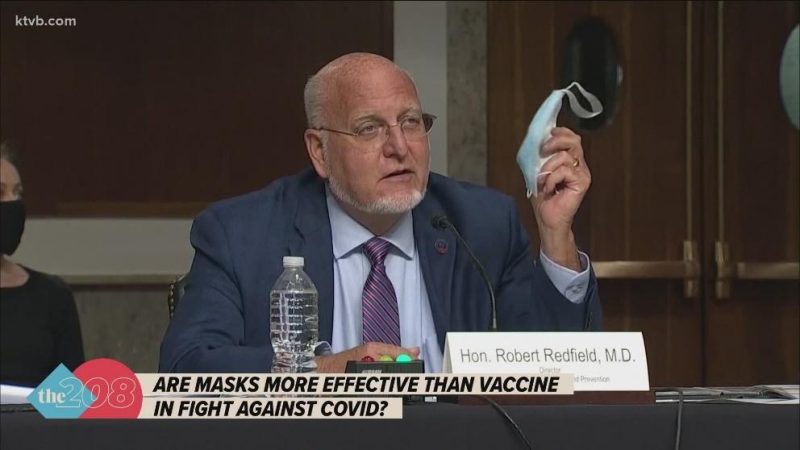
“We have clear scientific evidence they work. I might even go so far as to say that this face mask is more guaranteed to protect me against COVID than when I take a COVID vaccine, because the immunogenicity may be 70 percent and if I don’t get an immune response, the vaccine’s not going to protect me, this face mask will. Masks are the most important, powerful public health tool we have.”
He said that the pandemic would be brought under control if Americans embraced mask wearing for six to twelve weeks (just two more weeks!). He specifically called out 18- to 25-year-olds whom he said were responsible for continuing the outbreak in America. Mask-wearing was up to 90% in the United States and months later the seasonal wave hit, breaking through mask-wearing like a tornado through a hut. The picture doesn’t show it, but Redfield must have been wearing water skis under that table.
There’s a lot to unpack here. First, some percent of the population has natural immunity, what they call T-cell immunity, even prior to SARS-CoV-2 infection. We don’t know how much, but with so many people infected and asymptomatic (most of the infections), it could be 20-50% of the population. Second, the only way out of any pandemic is population, or herd, immunity. When a high percentage of the population acquires natural or vaccinated immunity, there just aren’t enough people able to pass it on, and it fizzles out.
If masks work, then why do individuals wearing masks need to quarantine if they were exposed to someone also wearing a mask? If masks offer better protection than a vaccine, then why were there capacity restrictions or closings of indoor dining when masks were required? Or, why were schools ever closed or allowed remote if teachers and students wore masks? Why did Sweden have a curve similar to other hard-hit countries without mask mandates, or any mask wearing?
The world had very high mask-wearing compliance. If masks were better than a vaccine, why didn’t it work? Anywhere? Dr. Redfield went on to say that vaccines were months away. President Donald Trump said that week that vaccines were three to four weeks away, and the media pounced on him for saying that. The first vaccine was announced as complete and ready to go one week after the election, seven weeks after Dr. Redfield’s statement.
In January 2021, some inventive middle-schoolers took some leftover mannequins from one of the retailers that went out of business because of the lockdowns. For their science project, they placed a surgical mask on a dummy head, and a cloth mask over it. Double masking. They declared it more effective than single masking (it probably was). Oh, one thing. It wasn’t some middle-schoolers. It was the CDC:

The second shark jump. We need to wear two masks. On February 11, 2021, Dr. Fauci told Savannah Guthrie on the Today show that “two masks are better than one, it’s common sense.” First, this recommendation by the CDC came nearly one year after the initial face mask recommendation.
We went from mask science-BC (before COVID-19) – that symptomatic individuals should maybe wear masks – to the CDC recommending everyone wear masks in March 2020, to them recommending two face masks for everyone, at a point when the hospitalizations were plummeting. How could a finding or recommendation like this take a full year?
There was no actual data that wearing two masks actually improved mask efficacy. In the mask-wearing universe, there were three segments of wearers: those that believed masks worked and wore them with great discipline; those that wore them whenever they were required, the rule-followers; and those that rebelled and either refused to wear them or wore them as little as possible, curbing their behaviors for a year to avoid wearing them.
The middle group lost confidence in the CDC and effectiveness of masks to protect against COVID-19. The CDC should have identified by late summer 2020 on that mask wearing wasn’t stunting the spread, that cases and hospitalizations in places with high mask usage weren’t doing better than the places without mandates.
CDC Study on Mask Efficacy
On November 27, 2020, the CDC released a mask study called “Trends in County-Level COVID-19 Incidence in Counties With and Without a Mask Mandate — Kansas, June 1–August 23, 2020.” The governor of Kansas issued an executive order requiring wearing masks in public spaces, effective July 3, 2020, which was subject to county authority to opt out. The study reported that “after July 3, COVID-19 incidence decreased in 24 counties with mask mandates but continued to increase in 81 counties without mask mandates.”

The study was released in late November but had a cutoff of late August. During the test period, COVID-19 hospitalizations in Kansas hovered around 300 a day against a capacity of 6,400, so about 5% of capacity. In October hospitalizations rose, like every state in their part of the country. By December COVID-19 hospitalizations hovered around 1,000 a day for several weeks, and then dropped sharply in January.
Below is what happened with absolute numbers of cases during the CDC study period:
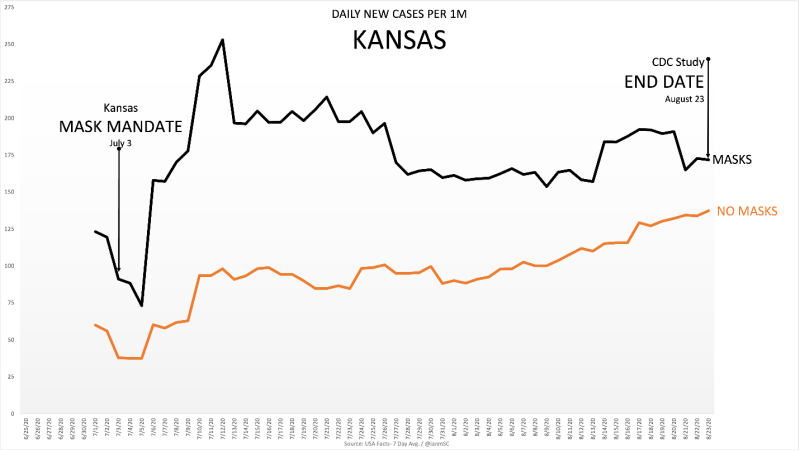
As you can see, the counties with mask mandates had more cases per capita than those without mask mandates.
Here’s what they did. Instead of comparing the case rate growth from July 3 when the mandate started, they chose to start by looking at the weekly case rate ending on July 9, after the masked counties had a huge increase. The seven-day average on July 3 was 91 per million. On July 9 it was 178 per million. They chose to start from 178.
What that allowed them to do was claim a 6% decrease since the mask mandate, because they got to ignore the 96% growth in the first week afterwards, giving themselves a higher baseline to start from. If you take the starting date of July 3 and the ending date of August 23, the case rate growth in the masked counties was 89%. If you start on July 9, it’s a 6% decrease.
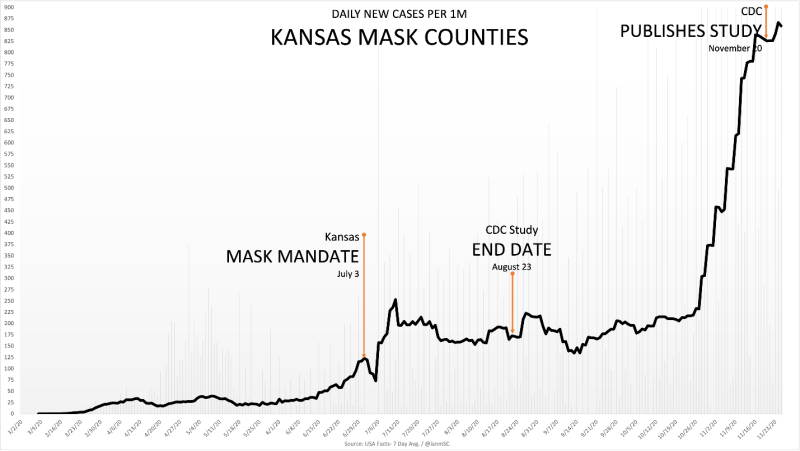
Further, you can see what happened to cases when the winter season hit the upper Midwest. The CDC cut off their study before the seasonal bump but released it well after cases rose. The CDC had this data but chose not to qualify their results, nor pull the entire study. Any time a study of this nature is completed and future data negates the conclusions, the study is scrapped. In this case it was released with no acknowledgement of what happened following the study period.
From the time the study ended through year-end, cases were about the same in the mask-mandated versus non-mandated counties. The burden is not on the non-masked counties to be better; having the same results nullifies the value masks are bringing to the table.
The CDC had this data for three subsequent months before releasing this study. I went to my primary care physician in December 2020 and we discussed masks. He mentioned this Kansas study. I asked him if he knew what the data was after the study cutoff date, and he did not. If there is one thing COVID-19 and the lockdowns should teach us, it’s that we should fact check data ourselves before running with anything provided from just one source.
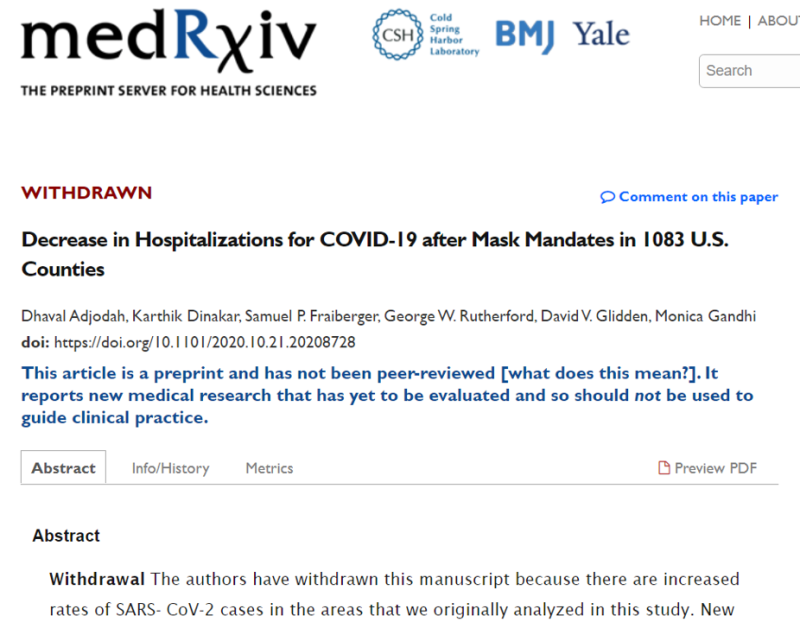
The CDC study should not have been released. Once released it should have been retracted like this study published in medRxiv. In 2020 a group of doctors conducted a study of the relationship between wearing masks and decreased hospitalizations in 1,083 counties in the U.S. It was published and then withdrawn because after the study, those counties increased hospitalizations invalidating their initial results:
CDC Jumps The Shark Again
Three days after Texas announced withdrawing their mask mandate, the CDC released this study: “Association of State-Issued Mask Mandates and Allowing On-Premises Restaurant Dining with County-Level COVID-19 Case and Death Growth Rates — United States, March 1–December 31, 2020.” Below are some key findings:
- Mask mandates were associated with decreases in daily COVID-19 case and death growth rates 1–20, 21–40, 41–60, 61–80, and 81–100 days after implementation.
- Allowing any on-premises dining at restaurants was associated with increases in daily COVID-19 case growth rates 41–60, 61–80, and 81–100 days after reopening and increases in daily COVID-19 death growth rates 61–80 and 81–100 days after reopening.
- Implementing mask mandates was associated with reduced SARS-CoV-2 transmission, whereas reopening restaurants for on-premises dining was associated with increased transmission.
How much of an increase was associated with not wearing masks or dining indoors? Twice as much? Three to four times more? Ten times more? To write a paper and publish it, it had to offer some very material differences in COVID-19 activity. They couldn’t jump the shark three times in six months, could they? If you play poker at all, you can relate to the expression that the CDC became “pot-committed.” They had invested so much in the lockdown pot that they had to see it through. On they went with these startling conclusions from their ten-month study on mask wearing and indoor dining:
- Masks were associated with a 0.5% decrease in COVID-19 cases in days 1-20 and 1.8% in days 21-100 following mask mandates in 2,313 counties (73% of all counties). 0.5% and 1.8%.
- Indoor dining was associated with a 1% decrease in COVID-19 cases
- Indoor dining was associated with ~2.6% increase in COVID-19 deaths
- “Mask mandates were associated with statistically significant decreases in county-level daily COVID-19 case and death growth rates within 20 days of implementation. Allowing on-premises restaurant dining was associated with increases in county-level case and death growth rates within 41–80 days after reopening. State mask mandates and prohibiting on-premises dining at restaurants help limit potential exposure to SARS-CoV-2, reducing community transmission of COVID-19.”
The CDC is stating that not wearing masks and dining indoors caused about a one percent increase in cases and thus drew the conclusion that everyone should wear masks and not eat inside a restaurant. Any freshman stats student could tell you that one percent is within a margin of error and not real-world-significant. They are further concluding that these NPIs contributed an additional 2.6% in COVID-19 deaths. It doesn’t pass the logic test.
Half the deaths were to people at life expectancy with multiple underlying conditions. These are not people going out to dinner. You can argue that people in contact with them could have caught it and passed it on to those at risk. That is possible. This is where you encourage those individuals to practice more personal responsibility, not close hundreds of thousands of businesses indefinitely.
Here are two New York Times articles that ran right after the CDC study:

The Washington Post ran this headline right after the Texas order.

In it, writer James Downie wrote, “The science is clear: As [Jake] Tapper noted, a new CDC study released last week found case numbers and deaths “slowed significantly” within three weeks of mask mandates being imposed, while eased restrictions on dining increase both cases and deaths.” That “slowed significantly” he referenced was the 1% decrease in cases. The media was shaping the fear in Americans. Rarely were major media outlets contextualizing the data or showing actual balance between COVID-19 health and public health.
Actual Face Mask Science After COVID-19
On May 25, 2021, Damian D. Guerra and Daniel J. Guerra published “Mask mandate and use efficacy in state-level COVID-19 containment” in medRxiv. This was the first study of U.S. data comparing mask efficacy and COVID-19 cases. Their conclusion was that case growth was not significantly different between areas that mandated masks and those that did not.
The researchers found higher mask wearing was not correlated to lower case growth rates, smaller surges, or less fall-winter growth at the end of 2020. They stated there is “inferential but not demonstrable evidence that face masks reduce SARS-CoV-2 transmission.” This means it feels like masks should’ve worked and done something, but there was no data to support that feeling.
When the CDC removed their face mask and social distancing recommendations for those vaccinated in May 2021, we thought pandemic restrictions were over. Prior to the announcement a third of the country was already completely mask-free. With the vaccines taking root and nothing adverse happening anywhere without masks, they caught up and called it a day. Almost. Most kids were still required to wear them if not vaccinated, and Dr. Fauci was still recommending them for school in the fall of 2021. They would catch up to reality and the mask-free states though.
With COVID-19 we had neither a category five (nor four nor three) pandemic nor very many interventions that worked. That this went on for two years wasn’t following the path of science, it was taking a detour with a machete cutting out new territory and ending up on the edge of a cliff.